INTRODUCTION
Every training and practising doctor
should become familiar with research processes and conduct, and where
possible have the opportunity to engage with research or pursue an
academic career as part of their professional choices.
1 However, in the UK, less than 10% of
doctors have a career in academia, at a time when the entire world has
woken up to the value of high quality research and researchers during
the current pandemic. Clinical academics play a vital role in advancing
our understanding and ability to treat existing and future
disease.
2 A diverse academic
workforce has been associated with greater scientific impact and
growth.
3 However, not all
individuals will progress in research and academia, with data showing
that in fact, diversity across clinical academics reduces as one
progresses through career milestones. Further analysis into diversity
demonstrates that a range of factors, (e.g. gender, race, disability)4
appear to contribute to limited progress in research and academia. In
recognition of these barriers to progression, the Research Excellence
Framework (REF) – (a system for assessing the quality of research in the
UK), places greater emphasis on organisations to demonstrate their
commitment to reducing inequality and increasing inclusivity. The Athena
Swan Charter was specifically developed to minimise the impact of gender
on career progression, with little doubt the programme did much to
highlight the problem of gender inequality in particular. All
stakeholders of research and academia have a statutory duty towards
reducing inequality and increasing inclusivity, including funding
bodies. In this paper, we explore the extent to which, publicly
available information shared by key grant awarding bodies, report on
outcomes relevant for career progression (or along research journey) in
academia, and across individuals with a range of protected
characteristics, with a focus on ethnicity among healthcare
professionals.
EQUALITY, DIVERSITY AND INCLUSION
(EDI)
Equality is defined as treating
people fairly, impartially and without bias and creating conditions
in the workplace and society that value diversity, promote dignity
and encourage inclusion.
5 Diversity is an inclusive concept,
concerned with creating an environment supported by practices, which
benefit the organisation and all those who work in or with
it.
5 Diversity takes account
of the fact that people, whilst similar in many ways, differ
including (but not exclusively) on the basis of gender, age, race,
sexual orientation, physical ability, mental capacity, religious
belief, education, economic status, personality, communication style
and approach to work.
5 Inclusivity
means that everyone feels able to be themselves, valued and safe to
express different ideas, comfortable in raising issues and
suggestions to others, knowing that this is encouraged, and being
creative to try different ways of doing things. There is more
awareness about equality, diversity and inclusivity following the
2010 Equality Act, which legally protects people from discrimination
in the workplace, and in society.
6
DIFFERENTIAL CAREER TRAJECTORIES
In the UK, a clinical academic career
involves a complicated training programme, with competitive multiple
entry points across Foundation, Core and Specialist training, some of
which, but not all, may be integrated within clinical training
programmes.
13 However, across
all these entry points, there are marked differences in success, for
individuals who identify with a protected characteristic - starting with
selection into programmes and success in obtaining funding awards. These
differences continue beyond training, and extend to career progression
as well as development opportunities, or achievement of senior academic
posts. The factors that contribute to disadvantage are wide ranging and
are commonly considered to interact with each other.
Gender
IThe Athena Swan Charter
14 was a system-wide programme to
address the structural inequalities facing women progressing with their
careers in science, technology, engineering and maths (STEM). As a
sector, higher education is relatively diverse, with almost equal
representation from men and women. However, the trend is different when
looking at contract type (fixed term vs. permanent) and appointment into
senior positions such as Readership and Professorships. These senior
positions in STEM were, and still appear to be male dominated (78.7%
male Professors)
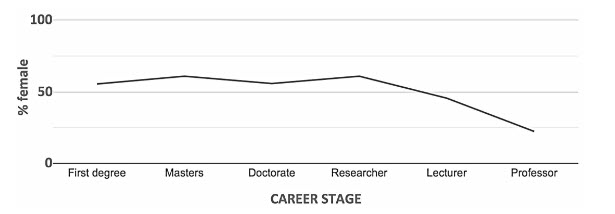
15 Although >50% of early career researchers are women
in clinical medicine and biosciences, the proportion drops dramatically
at more senior levels.
16
Figure 1. The Athena Swan Charter attempted to
reduce some of this gender disparity in a number of ways.17 The 2011
announcement by the National Institute for Health Research (NIHR) to
only shortlist clinical academic departments with a ‘silver’ Athena Swan
award for (certain) research grants, resulted in an increase in the
number of female clinical academics in senior positions.
14 An
independent review of impact suggested the Charter was successful in
bringing about cultural and behavioural change for the benefit of women
in research and academia, but questioned whether the pace at the ‘most
senior levels’ was fast enough.
14
Addressing inequalities, especially where factors operate at multiple
levels, is difficult and the success of the Charter to address these
challenges appears to have been limited. There is evidence that gender
inequality may have improved for White women academics but not
necessarily for Black, and minority ethnic women, and in some instances,
White women may now have an advantage over Black and minority ethnic
men.
15,18 Often, more than one protected characteristics could play a
role in attainment; for example there are less than 20 Black Professors
in the UK 19 thus the combination of multiple protected characteristics
causing greater barriers - also known as intersectionality - is
important.
20
Ethnicity
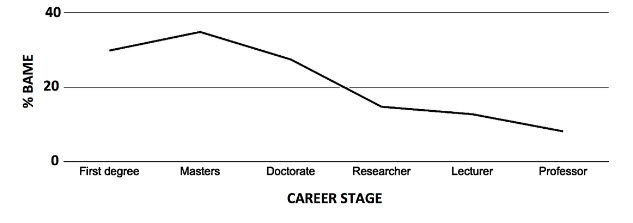
Although individuals from Black and
minority ethnic backgrounds make up 34% of the total population of
doctors, they account for less than 17% doctors in academia.
22,23 In terms of senior leadership positions held by
individuals from Black and minority ethnic backgrounds in the NHS and
academia, the evidence demonstrates a lack of representation in both
contexts.22 Likewise, individuals from Black and minority ethnic
backgrounds are also under-represented across most levels in academia,
suggesting significant barriers still exist around progression along
career pathways
Figure 2.
The lack of representation appears to
extend across different institutions and organisation within research
and academia. Diversity data from the Research Council 2018 shows that
84% of the academic population in the Medical Research Council (MRC)
identify as White, with 4% and 1% belonging to Asian and Black
backgrounds, respectively. Further, 79% of the student population at MRC
was from a White ethnicity despite most medical schools having greater
proportion of their cohort, made up of individuals from Black and
minority ethnic backgrounds.
Success rates for principal
investigator funding across MRC grants and awards in 2016-17,
demonstrated a higher proportion of applicants identifying as White
(24.1%) compared to successful applicants from Black and minority ethnic
backgrounds (16.3%). Data describing successful new investigator
research grants from 2017-18 demonstrated higher success rates for
applicants identifying as White (24%) compared to applicants from Black
and minority ethnic backgrounds (7%).
24
Data from UK Research and Innovation (UKRI) in 2019 suggest the gap may
be widening with a higher success rate observed again among individuals
identifying as White (27%) compared to those identifying as Black and
minority ethnic (17%).
Data from the Wellcome Trust on grant
funding awards, identified the majority of successful applicants
identify as White (87%), and there was a consistent gap in success rates
over a three-year period between 2016-2019. Across this data, Black and
minority ethnic applicants were also under-represented among those who
were successful at obtaining more senior awards and fellowships.
25 Furthermore, the odds of non-White
applicants receiving funding were 0.68 times those of White
applicants.
25
The Higher Education Statistics Agency
(HESA) suggested that 91.2% Professors identified as White compared with
3.5% who identified as Asian and 0.6% who identified as Black.
15 Only 3.2 % of Heads of the
Institutions identified as Black and minority ethnic. Students from
Black and minority ethnic backgrounds were also less likely to progress
to scientific jobs after graduating than students identifying as
White.
16
Other protected characteristics
Reporting of outcomes from individuals
with protected characteristics can be limited due to need for protecting
anonymity when group sizes are small. Individuals with visible and
non-visible disabilities are under-represented in a range of work
settings, and the trend is no different in the scientific
workforce.
16 Only 2% of
UK-based applicants for Wellcome grants declared a disability at the
point of application (19% of working-age adults are disabled according
to the UK Government family resources survey 2016/17). There is some
data to suggest that people with a disability have less success at grant
award rate (13% versus 15%).
25 Although
not strictly a protected characteristic, deprivation is associated with
poorer outcomes especially among individuals with protected
characteristics. Individuals from a lower socio-economic backgrounds,
irrespective of ethnicity, are less likely to enter research and
academia, and are also less likely to progress in their careers as well
as take longer to get to professional level
16 Similarly, 2017 data from the Wellcome Trust,
suggested inequalities in entry to doctoral studies due to
socio-economic background, despite same attainment level in graduate
studies.
26
Protected characteristics and
intersectionality
Table 2: Funders represented
within the reports (see Appendix 2)
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
19 |
| Ethnicity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Gender |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Age |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Socioeconomic
Background |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Table 2: In the
table above, the Blue colour shading signifies presentation of data
about the specific protected characteristic in the published report. The
Orange colour shading signifies the absence of data about the specific
protected characteristic in the published report. Reports here are
listed as 1-19; see
Appendix 3 for a full
named list of reports included. Gender was the most common protected
characteristic for which outcome data was presented (79%), followed by
ethnicity (53%), disability (21%) and then both age and socioeconomic
background (11%). Other protected characteristics, such as sexual
orientation, disability and religion were not specifically evaluated
across any of the reports.
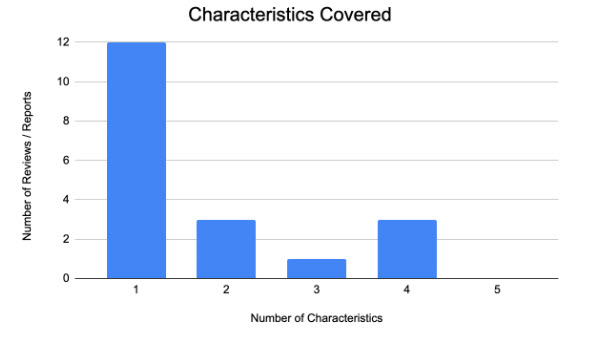
All 19 reports covered one or more of
four protected characteristics – gender, ethnicity, disability, age and
socioeconomic background
Table 2 . However, only
a few reports focused on more than one protected characteristic
Figure 5. Seven reports covered two or more
protected characteristics, whilst 4 reports covered three or more
characteristics, and only 3 reports covered four or more
characteristics. None of the reports covered more than five protected
characteristics.
Mapping of data from reports to factors
identified in the Bridging the Gap 2020 Thematic series.
27
Data identified from the 19 reports (see
Appendix 3) that mapped onto factors from
the Bridging the Gap 2020 Thematic series
27 associated with DA is presented below
Table 3.
Table 3:, The
colour Blue signifies presence of a factors from the Bridging the Gap
2020 Thematic Series.27 that were
presented in a published report. The colour Orange signifies absence of
any of those factors presented in a published report. Reports here are
listed as 1-19; see Appendix 3 for a full
named list of reports included.
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
19 |
Total yes |
| Educational |
|
|
| Learning styles (problem
based/ taught/ self-directed) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Access to resources,
guidance or tutoring |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
| Schooling (independent
or state) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Impact of economic
status on educational opportunity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Parental/ family
(influence of parental education, support, expectation
or motivation) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Assessment (multiple
choice, viva, observed clinical assessments) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Impact of unrecognised
dyslexia or dyspraxia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Cultural |
|
| Linguistics (IELTS) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Previous life
experiences |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Conflict/ refugees |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Societal norms/
expectations (introvert vs extrovert) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Influence of reverence
of those more senior/in authority |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Segregation (wilful or
forced) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Bias |
|
| Segregation (wilful or
forced) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19 |
| Impact of illness or
health impairment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Support |
|
| Family, friends |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Formal supervision |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Mentorship |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Networking |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Economic |
|
| Deprivation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Access to bursaries |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
| Cost of examinations/
preparation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Family responsibilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Others |
|
| Health (physical/
mental) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
| Immigration related
stresses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Wellbeing, Stress and
Burnout |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| Caring responsibilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
All reports documented the impact on
outcomes from factors such as age, disability, race and socioeconomic
status on the immediate outcomes in research and academia such as
failure to obtain a successful award or progress in a career. However,
no reports explored the subsequent short- or long-term impact of these
factors on the personal well-being, or physical and psychological health
outcomes of individuals, as a potential risk factor for further or
future disadvantage. Among the educational factors associated with
differential career outcomes,
27 access
to resources, guidance or tutoring were reported in 6 reports (32%).
Learning styles, schooling type, impact of economic status on
educational opportunity and impact of potential unrecognised
dyslexia/dyspraxia were only mentioned in one (5%) report.
Among the cultural factors associated
with differential outcomes,
27 no
reports investigated the role of linguistics, conflict/refugee status or
segregation as a cause for DA in a research or academic context. Four
reports noted the influence of accessing support from a senior (21%) and
2 reported noted societal norms/expectations (11%). No reports
investigated the impact of limited networking opportunities in a
research and academic context. Four reports (21%) investigated the
availability of formal supervision and 6 (31.6%) mention accessibility
to mentorship as contributing factors.
Among the economic factors associated
with differential careers,
27 the impact
of deprivation, access to bursaries, cost of examinations/preparation
and a family responsibility was investigated in part. Access to
bursaries was reported in 3 reports (16%), with family financial
responsibility reported in 2 reports (11%). Deprivation and cost of
exam/exam preparation were also reported on one occasion.
Within the factors classed as “other”
were immigration related stresses, wellbeing/stress/burnout and caring
responsibilities.
27 Immigration
related stress was not reported on as a potential driver of differential
carers. Health and wellbeing/stress/burnout was only reported on in 2
reports (11%). That said, caring responsibilities was reported in 7
reports (37%).
DISCUSSION
This rapid scoping review was
undertaken to evaluate the extent to which funding bodies reported
equality, diversity and inclusivity outcomes, with a specific focus on
evidence of DA among individuals with protected characteristics and the
impact of intersectionality among individuals from Black and minority
ethnic backgrounds. The findings demonstrated DA across funding body
outcomes is also prevalent, and the impact of multiple protected
characteristics (e.g. gender and ethnicity) appear to particularly
amplify the achievement gap between Black and minority ethnic and white
individuals in research and academia. Furthermore, the mapping data
presented in the published reports with factors associated with DA
identified in the Bridging the Gap 2020 Thematic Series document
27
demonstrate an ‘awareness gap’ between funding bodies and individuals
from Black and minority ethnic backgrounds about barriers to success as
well
Table 3. The findings from the review
highlight a number of issues that need further exploration and
discussion with all stakeholders of research and academia in the
UK.
Broadening the EDI lens to consider the full range of career limiting
factors
Firstly, there is a need to reflect
over the starting point for this scoping review and the lens through
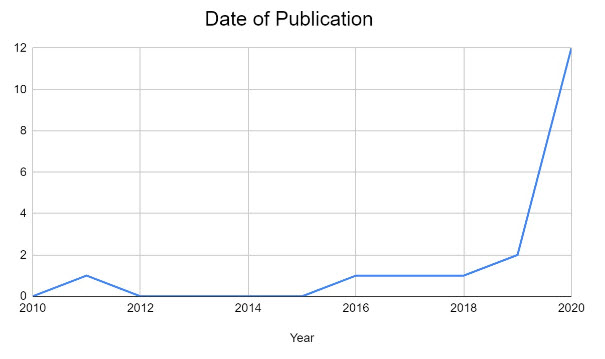
which it was undertaken – equality, diversity and inclusivity (EDI).
Although the review demonstrated greater awareness of EDI over the last
decade, many of the reports have only been conducted in the last year or
so, and thus few reports have been able to be repeated, to evaluate
change in outcomes. Likewise, across many reports, gender outcomes have
been the focus of improvement, but in some respects, gender appears to
have been conflated with EDI in the broadest sense, more so than
ethnicity or disability. This foregrounding of gender over and above
other protected characteristics is multifactorial and likely includes
interventions by funders such as NIHR after 2011, stipulating specific
conditions related to gender targets before awarding funding to
organisations.
14 This is perhaps unsurprising given the
focus on gender through statutory gender pay gap reporting since 2017,
and the Athena Swan Charter. This target-driven approach has led to
positive change with respect to actions to progress gender equality,
though outcomes are still far from equal, especially at senior levels.
Conversely the danger of focusing on one particular characteristic over
another is the risk of fuelling a sense that one group's injustice is
more or greater. For this reason, there is a real need for funders and
stakeholders to consider all programmes of work on EDI within their
organisations, and to evaluate the extent to which they acknowledge
individuals across the range of protected characteristics.
Another reason for the focus on gender
rather than other protected characteristics such as ethnicity, may
involve a degree of blindspot bias.
50 Given the lack of general
awareness and/or data collection about EDI within research and academia,
conceptualisations of inequality among funding bodies appear to focus on
gender rather than being fully inclusive of individuals belonging to
groups with all protected characteristics. Further, this general bias as
a whole appears to have led to a general lack of recognition about
broader EDI issues, especially for people from Black and minority ethnic
backgrounds.
51,52 In fact, the notion of ‘White privilege’ was not
reported in any report further suggesting a lack of awareness, or
understanding about this concept despite the recognition of it in the
wider literature,
53 despite many higher education institutions
committing to Advance HE’s Race Equality Charter (REC).
54 The same is no
doubt true for other protected characteristics where there are workplace
initiatives to advance inclusivity such as Disability Confident and
Stonewall Diversity Champions. This is perhaps due to fatigue of one
program but also not having similar linked intervention by funders such
as NIHR for Athena Swan Charter.
14
The interaction of different protected characteristics should be
focal in advancing inclusive research and academic careers for
doctors
Secondly, and related to the concept of
protected characteristics, is the notion of intersectionality
20 Defined as 'the interconnected
nature of social categorizations such as race, class, and gender as they
apply to a given individual or group, regarded as creating overlapping
and interdependent systems of discrimination or disadvantage’,
intersectionality is a particular issue for individuals from Black and
minority ethnic backgrounds but also is important for individuals from
White backgrounds. Although well described in wider literature to date,
the issue of intersectionality was conspicuous by its absence among
research and academics in this review. The problem appears to strike a
chord among Black and minority ethnic doctors when describing their
experiences of overcoming barriers in research and academia. For
example, whilst addressing gender inequality, will no doubt help Black
and minority ethnic women progress in research or academia, there is
little doubt that Black and minority ethnic women also face additional
barriers as a consequence of their ethnicity. Put another way, ethnicity
was one less barrier non- Black and minority ethnic women had to face,
or one more barrier Black and minority ethnic women had to face in order
to advance in research and academia. However, the general lack of
understanding or acknowledgement of the problem demonstrated across
reports suggests much progress needs to be made in this area.
Many of the reports focused on factors
such as gender, ethnicity, disability, age and socioeconomic background.
These factors were most likely chosen because they are easy to measure,
given many funders and stakeholders already have this type of data. The
usefulness of this data is limited for a number of reasons. Ethnicity is
often used as a catch all term for any individuals from Black and
minority ethnic backgrounds, and ignores the observation that there is
as much, if not more variation between different Black and minority
ethnic versus non-BAME backgrounds. Outcomes in higher education are not
to be the same for Black people or people who self-identify as
Bangladeshi or Pakistani, as compared to people who self-identify as
Indian, British Indian or Chinese, with the latter achieving better
outcomes on some measures than the reference non-BAME group.
55 The homogenisation of individuals
from Black and minority ethnic backgrounds into one ethnic category does
little to acknowledge the significant variation among people in this
group, as well as their specific perceived barriers in research and
academia. This form of categorisation can also lead to reductionist
interventions to mitigate the impact of unconscious bias are undermined
since the problem - ethnicity - has been oversimplified to the point
where it doesn’t really mean anything that matters. Whilst there is an
acknowledgement that the numbers may preclude meaningful analysis in
variation, and so some aggregate data is required, more transparent and
considered analysis is required. Hence, future analysis using
disaggregated ethnicity categories (for both Black and minority ethnic
and White) would highlight where the widest gaps are.
The need to acknowledge personal and socio-cultural factors may
influence the BAME attainment gap in ways non-BAME groups may not
fully understand so should take time to do so
Prior to this review, the Bridging the
Gap programme of work highlighted many possible factors which impact
differential outcomes in dual academic and research careers for
doctors.
27 These factors are
span multiple domains including education, culture, and social
circumstances, yet many of the reports reviewed in this paper did not
appear to acknowledge their existence or effect on progression for
doctors from Black and minority ethnic backgrounds. For example, none of
the reports acknowledged the significant positive influence of parents
and family on the motivation levels and resilience among doctors from
Black and minority ethnic backgrounds. Instead beyond the research and
academic context, there has been negative stereotyping that
characterises the families of Black and minority ethnic doctors as
coercive and demanding on individuals.
56 Despite there being a large body of literature
demonstrating the value of parental or family support to individuals for
achieving many academic and non- Black and minority ethnic doctors
appear not to be provided specific support with linguistics even when
there is evidence sophisticated communication support and coaching may
improve outcomes for Black and minority ethnic doctors at
assessment.
57 In contrast, when
individuals with specific learning require support due to various
information processing challenges they face, organisations are prepared
to fund it without too much delay. When Black and minority ethnic
doctors struggle with language, dialect and academic writing, the
perceived response is often for individuals to work harder or attend
extra training rather than a form of developing coaching or performance
enhancement intervention,
58 thus
focusing on the deficit model rather than looking at wider institutional
change. Even for some factors such as immigration and visa related
issues, particularly unique to non-UK Black and minority ethnic doctors,
there was no acknowledgement of this challenge as a factor affecting
research and academic outcomes, demonstrating the general lack of
awareness or blindspot among funders and stakeholders about these
problems.
Avoiding simplistic population or BAME-based interventions for
overcoming barriers related to attainment gap
The findings from the review demonstrate
the very real gap between the perceptions of individuals from Black and
minority ethnic backgrounds about the factors preventing them from
achieving their full potential, and the focus of stakeholders such as
funding bodies about drivers of progression in research and academia and
their role in addressing this. Interventions for addressing EDI issues
seem to focus on the ‘bias’ as the main cause of the doctors from Black
and minority ethnic backgrounds progressing in their careers. Although
de-biasing interventions are well-reported in the wider literature,
their effectiveness for improving individual outcomes for doctors from
Black and minority ethnic backgrounds remain unclear. Furthermore,
de-biasing interventions or unconscious bias training assume that ‘bias'
is something that can be trained out of those who demonstrate it. The
extent to which there is evidence that such strategies are able to
achieve this outcome in any meaningful or long-term way is also lacking.
Conversely, doctors from Black and minority ethnic backgrounds who
report being subject to forms of bias, are often referred to
communication, leadership or resilience training courses. The assumption
underpinning all of these interventions is that individuals can be
trained to become resilient to the problem however there is little
evidence in the wider literature for effectiveness of these approaches
either. These types of organisational interventions or responses infer a
deficit model within the individual rather than acknowledgement by
funders and stakeholders of a problem within the system being the cause
for poorer outcomes in research and academia among doctors from Black
and minority ethnic backgrounds.
Moving away from EDI ‘projects’ to sustained and embedded practice
Many of the reports included in this
review also appeared to detail single pieces of work or projects related
to EDI, rather than a long-term programme of work committed to achieving
change in research or academia for individuals with protected
characteristics. This scoping review evidenced elements of positive
practice from funders about their focus on EDI, mostly in relation to
gender, but the opportunity now exists for widening the breadth and
depth of those EDI programmes of work. Whilst there was a particular
absence of attention towards intersectional factors that could be career
limiting, the findings from this review may help develop specific,
measurable actions that can help to reduce DA in a meaningful way. The
success of narrowing gender disparity was likely driven by a statutory
focus on the gender pay gap reporting as well as the Athena Swan
Charter. There is now an opportunity to fully embrace and embed the REC
into policy making at all levels across research and academic
environments.
MOVING FORWARD
As a result of this review, a number of
areas have been identified for further discussion with funders and
stakeholders in small-group workshops to guide further research and
policy developments.
The collection, analysis and sharing of
data relating to progress in research and academia for people with
protected characteristics
Possible areas for exploration
include:
- Creating a uniform framework of what EDI data should be
collected by stakeholders and organisations including funding
bodies
- Longitudinal reporting of outcomes for all people, including
those with protected characteristics from selection into
academic training pathways through to grant/funding awards and
career progression
- Working together with HEIs and NHS Trusts to develop a
framework for monitoring their own data and ensure reducing the
attainment gap is a priority
- Meaningful reporting of data analysis incorporating effect of
intersectionality and multiple protected characteristics as
compared to single or few.
- Likelihood of COVID19
The development of EDI strategy that is
inclusive for all, and not just exclusive to the few
Possible areas for exploration
include:
- EDI strategy development that accurately reflect the challenges
faced by people across the range of protected characteristics
- EDI strategy that includes training of staff to raise awareness
about the barriers faced by people with protected
characteristics, e.g. BAME doctors as reported in the wider
literature
Representation from people with
protected characteristics across leadership and management structures
Possible areas for exploration
include:
- Efforts to increase representation from people with protected
characteristics feeding into committees and decision making
policy within your organisation
- EDI strategy that includes training of staff to raise awareness
about the barriers faced by people with protected
characteristics, e.g. BAME doctors as reported in the wider
literature
- Positive action to accelerate the pace at which representation
is improved at senior academic and research levels e.g. targeted
fellowships for mid-career etc.